Knee Replacement: Regain Mobility and Live Pain-Free
Are you struggling with joint pain while walking, climbing stairs, or doing daily activities?
Do you have osteoarthritis, a joint injury, or stiffness that limits your movement?
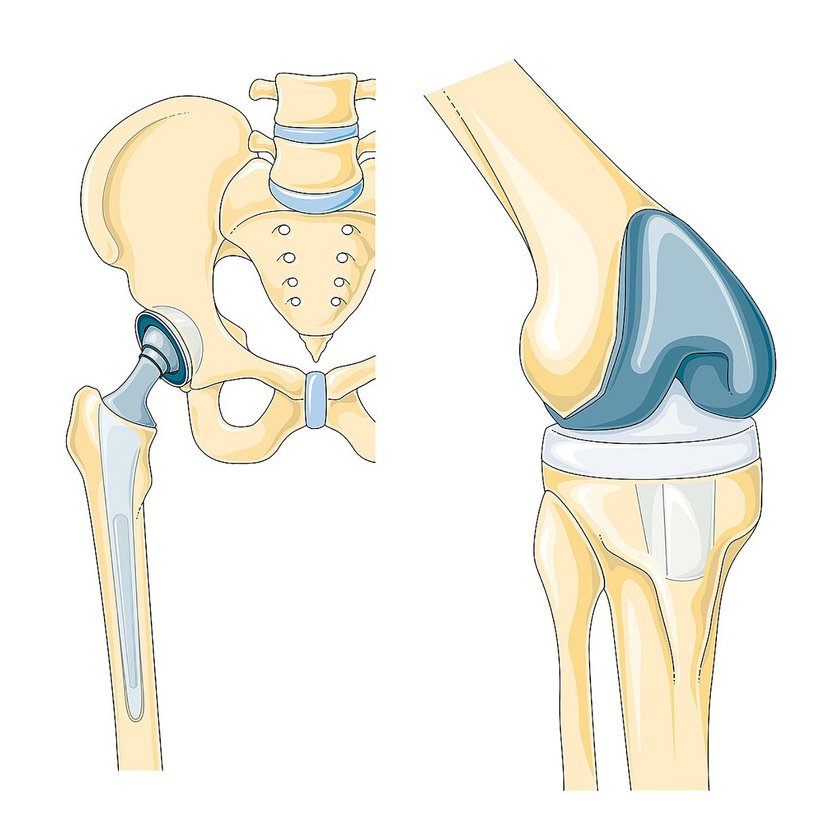
If yes, knee or hip replacement surgery may be the right solution for you.
Dr. Debabrata Padhy is one of the most trusted orthopedic surgeons in Bhubaneswar, known for his expertise in joint replacement surgeries, especially knee and hip replacements. With years of experience and a compassionate approach, he has helped hundreds of patients regain their independence and lead pain-free lives.
At his clinic, patients receive personalised evaluation and advanced surgical care focused on long-term joint health and improved mobility.
The preoperative evaluation generally includes a review of all medications being taken by the patient. Anti-inflammatory medications, including aspirin, are often discontinued one week prior to surgery because of the effect of these medications on platelet function and blood clotting. Other preoperative evaluations include complete blood counts, electrolytes (potassium, sodium, chloride), blood tests for kidney and liver functions, urinalysis, chest X-ray, EKG, and a physical examination. Your physician will determine which of these tests are required, based on your age and medical conditions. Any indications of infection, severe heart or lung disease, or active metabolic disturbances such as uncontrolled diabetes may postpone or defer total hip joint surgery.
Total hip joint replacement can involve blood loss. Patients planning to undergo total hip replacement often will donate their own (autologous) blood to be stored for transfusion during the surgery. Should blood transfusion be required, the patient will have the advantage of having his or her own blood available, thus minimizing the risks related to blood transfusions.